
Effectiveness, Proportionality, and Dignity: Three Standards for Good Patient Monitoring
The statement of the Swiss Academy of Medical Sciences and the Federal Council’s response provide clear guidance.
Two statements, one direction. The Federal Council and the Swiss Academy of Medical Sciences (SAMW) have addressed the issue independently.
In its response to a parliamentary interpellation, the Federal Council examines less intrusive forms of monitoring. It names systems that do not continuously process image and sound, and it explicitly names the radar sensor. The SAMW states the same principle: collect as little data as the purpose requires. It commends data-minimising, image-free approaches.
Monitoring systems that do not work with image data (but, for example, with radar) are to be preferred, in line with the principle of data minimisation. (SAMW, Central Ethics Committee statement, Digital monitoring in inpatient and long-term care)
For decision-makers, this is no longer an academic question. It is a signpost for procurement. Whoever selects a system today has a clear standard to follow.
Proportionality complements effectiveness and innovation. It is the third pillar of QUMEA’s philosophy. It means the least intrusive impact on workflows and on the integrity of staff, patients, and relatives.
The starting point must always be the individual patient’s needs
QUMEA starts with the individual patient. Monitoring is justified when it is suitable and necessary for this person. That is the core of proportionality. It is also the SAMW’s position: an individual indication rather than blanket routine.
QUMEA focuses where the fall risk concentrates: at night, and among cognitively impaired or otherwise vulnerable people. Falls often happen when someone tries to leave the bed, or around going to the toilet. A good system is therefore embedded in the risk assessment and simple to use.
Dignity is built in, not retrofitted
Once the monitoring fits the individual case, the next question follows: how deeply does it intrude on privacy? Dignity cannot be configured after the fact. It is decided in the architecture and technology of the system, long before the first setting is made.
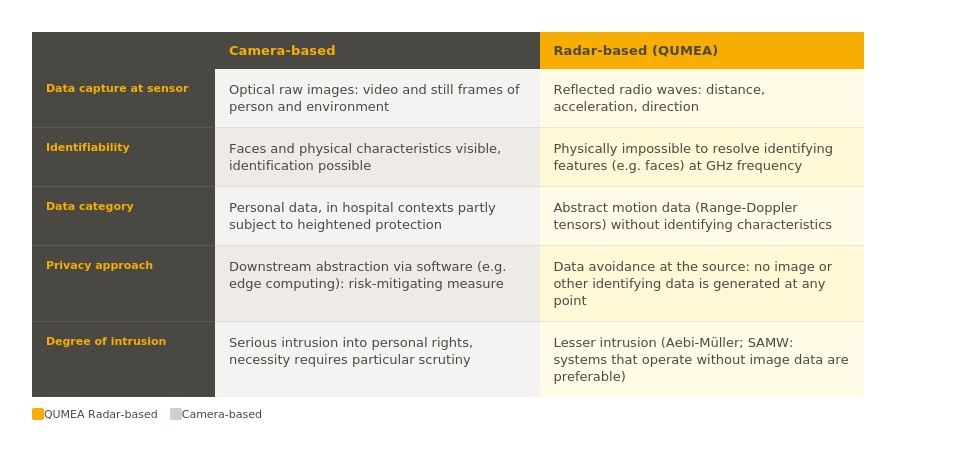
QUMEA uses radar. At the point of data capture, only abstract movement data arise: distance, motion via the Doppler frequency shift, and direction. No images are created. Radar operating in the GHz frequency range physically cannot resolve faces. What was never captured cannot be reconstructed, even with the best software.
QUMEA avoids the image from the outset, rather than blurring it afterwards. No personally identifiable data are generated in the first place. This is data minimisation at the source. It meets the requirement of necessity, which demands the mildest suitable means.
The expert discussion points the same way. According to Regina E. Aebi-Müller, Professor of Law at the University of Lucerne and Chair of the SAMW working group that prepared the statement, radar-based systems interfere less with patients’ personality rights than other forms of digital monitoring. The SAMW statement is available as a PDF download at the end of the original article (in German).
Less intrusive methods are especially considerate of patients with cognitive impairment, whose capacity to decide is often no longer present. The literature therefore classifies a system’s intrusiveness as a clinically relevant parameter (Lahr et al., Sensors 2025).
Effective, with few false alarms
Data minimisation only helps if the system also works. Effectiveness shows in the clinical result: does the system demonstrably reduce falls? This proof must meet scientific evidence standards, that is, be established in a clinical study, not in manufacturer claims. Behind it lie two questions: does the system reliably detect risk situations? And how often does it raise an alarm without cause?
The clinical benefit is supported by a controlled study. The QumPreFall study at the DelirUnit of the University Department of Geriatric Medicine Felix Platter compared QUMEA directly with the bell mat, the previous standard, in 119 patients with delirium. It is registered (clinicaltrials.gov, BASEC), approved by the responsible ethics committee (EKNZ), and currently in peer review. Under QUMEA, the fall rate fell significantly, by about 50 percent compared with the bell mat. At the same time, the bell mat produced significantly more warnings and kept nursing staff at the bedside significantly longer (Hasemann et al., 2024).
False alarms burden nursing staff. This is exactly where QUMEA delivers solid figures (Eichenbrenner et al., 2024). In a study on a delirium ward, the most challenging patient group, the system produced exactly one false alarm across 18,438 observation windows without a fall. The positive predictive value (PPV) was 96%. For a team at the bedside, that means hardly any unnecessary alarms.
This finding is supported by further practical evidence from Swiss long-term care. In one facility, the fall rate fell over 18 months from 5.6 to 2.2 falls per resident per year, a decline of about 60 percent. This is an observed trend, not a controlled study. During the same period, the facility moved into a new building, which also influenced the figure. We therefore do not attribute the decline to QUMEA alone. What the study does show with certainty: the nursing team’s trust in the alarms rose from 46 to 73 percent (Schneider et al., 2026; in German).
Nightly routine checks fell from three to two rounds per resident. That creates time for individual care.
Simple technology, substantial benefits
Protecting staff is a principle in its own right. The SAMW and the Regional Ethics Group Zurich (in German) name it explicitly. A good system does not assess the work of the nursing staff. It steps back during care activities.
In 2025, QUMEA surveyed around 800 nurses in five countries. 94 percent consider it important that a monitoring system processes no images. That supports the chosen path.
QUMEA identifies no individuals and captures no image. It signals risks, gives nurses calm, and strengthens trust within the team.
Innovation, proven rather than claimed
QUMEA drove radar-based, image-free monitoring early, when the idea was still the exception. The pioneering role, with more than 7,000 monitored patients across nine countries, is not an end in itself. It shows that the data-minimising approach works in everyday clinical practice today.
The SAMW requires that the benefit be proven through piloting with clear quality indicators. QUMEA takes exactly this path, rather than relying on plausibility. The evidence spans signal quality, alarm accuracy, and demonstrated clinical outcomes in practice. It is growing across several facilities, countries, and patient groups.
Conclusion
In the end, it is about the dignity of the patient. The SAMW holds that, alongside the protection of data, human dignity must be considered in a differentiated way. It means moments of particular intimacy: personal hygiene, emotional crises, the dying phase.
Dignity begins with the question of what is captured at all. That is where QUMEA stands: no image, no lens, no intrusion into the intimate sphere that cannot be taken back. This protects patients in their most vulnerable moments, and at the same time relieves the people who accompany them.

Together with the Landeskrankenhaus Hall | Tirol Kliniken GmbH: An authentic glimpse into everyday nursing care
An authentic glimpse into clinical daily life shows how QUMEA supports nursing professionals. The anonymous, contactless technology creates more safety without unnecessarily interrupting daily care routines, while consistently protecting data privacy and confidentiality.

VGR and QUMEA: An interview on one of Europe's largest radar projects
Falls in hospitals rarely happen without warning. The changes that precede them, in mobility, in restlessness, in how a patient moves through the night, often go unnoticed between routine checks. This is the gap the Västra Götaland Region (VGR) set out to close when it began one of the largest publicly tendered movement monitoring projects in Europe.

QUMEA appoints Elad Benjamin as Chairman of the Board
Benjamin brings more than 25 years of experience in healthcare technology, enterprise software, and AI-driven medical solutions to support QUMEA’s next phase of growth.